Inpatient mental health services are designed to be safe havens for individuals grappling with mental health challenges, providing essential support and recovery opportunities. Unfortunately, many patients report experiences that starkly contrast this ideal, often sharing distressing accounts involving restrictive practices such as seclusion and restraint, coercion, and overwhelming boredom. These negative experiences can exacerbate trauma, making recovery a more arduous journey. Such critical issues have been extensively discussed on the Mental Elf platform, highlighting the experiences of diverse age groups, including children and adolescents in inpatient services.
To foster improvement in inpatient mental health care, it is imperative to gain a comprehensive understanding of patients’ negative experiences. This knowledge will enable us to devise effective strategies to address these challenges. Previous reviews have delved into specific negative experiences, such as the impact of surveillance technologies on wards or the effects of risk management practices. Additionally, some studies have honed in on marginalized groups, particularly black service users, who face systemic racism within mental health care systems.
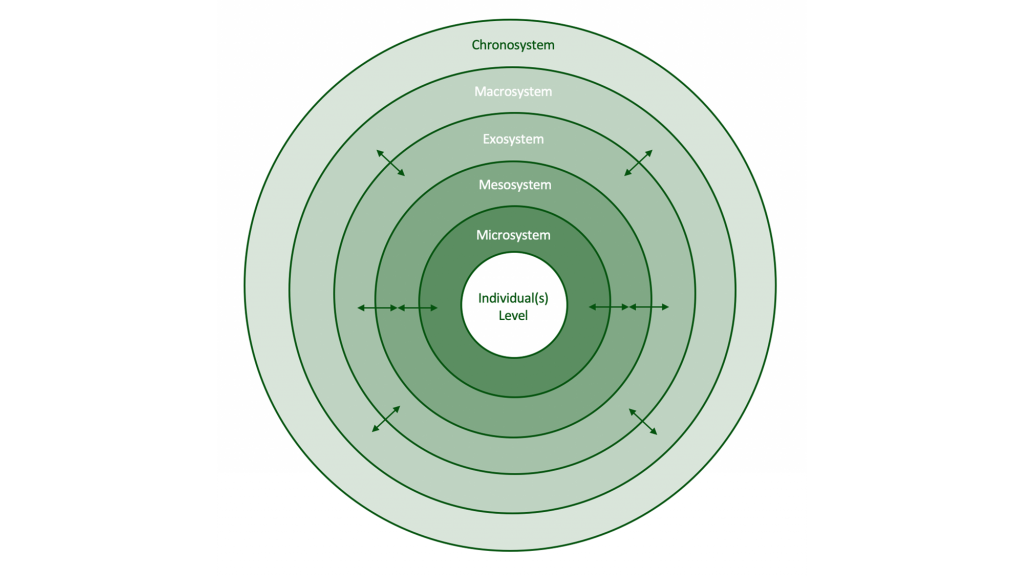
A groundbreaking qualitative systematic review conducted by Hallett et al. (2024) represents a significant advancement in this area, as it broadens the scope of inquiry by examining the full spectrum of patients’ adverse experiences within inpatient mental health settings. This review uniquely incorporates Bronfenbrenner’s ecological systems theory (1992), which posits that an individual’s experiences are influenced by various environmental layers, from immediate surroundings to broader societal contexts.
By systematically mapping how these environmental layers contribute to adverse experiences in mental health wards, the review provides valuable insights that can inform and enhance service design and delivery. The ultimate goal is to improve patient care and outcomes, ensuring that individuals receive the support they need in a nurturing and safe environment.
This was the first review to explore the full range of adverse inpatient experiences and the first to apply Bronfenbrenner’s ecological systems theory.
The researchers undertook a systematic review of qualitative studies focused on patients’ adverse experiences in acute adult, forensic, and psychiatric intensive mental health inpatient care, deliberately excluding specialized settings such as those catering to children and young people, older adults, or individuals with learning disabilities. This focus ensures a more nuanced understanding of the experiences within specific inpatient contexts.
To identify relevant studies, the research team conducted searches across three academic databases and Google Scholar. They meticulously extracted data, ensuring thorough checks and quality assessments of the studies using the Critical Appraisal Skills Programme (CASP) checklist, which is a recognized tool for evaluating research quality.
A “best-fit” framework was utilized to systematically organize the qualitative findings from the included studies. This approach began with themes grounded in existing knowledge and was refined as new insights emerged during the analysis, providing a robust structure for understanding the data.
Notably, the research team included a member with lived experience of inpatient mental health care, who contributed to all stages of the review process. Additionally, feedback was sought from a Patient and Public Involvement group comprised of five service users, each with diverse experiences in acute and secure inpatient mental health care. This collaboration ensured that the review accurately reflected real patient experiences, emphasizing the importance of including diverse perspectives in research.
The team included a researcher with lived experience of inpatient mental health care and gathered feedback on preliminary themes from a Patient and Public Involvement group.
The review ultimately included 111 papers, which employed a variety of methodologies and were predominantly rated as good quality. While the studies encompassed a global perspective, most of the research was conducted in Europe (n = 80), underscoring the need for a broader understanding of adverse experiences across different geographical contexts.
This systematic review uncovered a multitude of factors contributing to adverse inpatient experiences, revealing that traumatic incidents within mental health inpatient settings can significantly deteriorate patient outcomes. These adverse experiences were categorized under three primary themes: the ecosystem, systems, and the individual.
Understanding the Ecosystem: The Role of Environment in Adverse Experiences
The term ‘the ecosystem’ encompasses the physical environment and available resources in which adverse experiences unfold, alongside the interactions with people who inhabit or influence that environment. Adverse experiences often stem from the physical conditions of the ward, which may include poor environmental factors such as overwhelming sensory stimuli, including loud noises and incessant alarms. A lack of engaging activities can lead to significant boredom, while patients may perceive the wards as unsafe, resembling prison-like settings due to rigid rules and constant surveillance. Additionally, interactions with others—primarily ward staff, but also fellow patients and family members—play a crucial role in shaping negative experiences. Contributing factors include insufficient staff numbers, a culture of staff invisibility in communal areas, lack of information sharing, exclusion from decision-making regarding personal care, and negative staff attitudes, which may encompass stigma and racism towards patients.
Evaluating Systems: The Impact of Treatment Processes on Patient Experience
The term ‘systems’ refers to the formal treatment processes, which can include coercive management strategies such as seclusion, restraint, and threats of involuntary detention. The use of psychotropic medications and the monitoring of patient progress during ward rounds are also integral components of these systems. Many participants felt that these processes were punitive, often inducing fear and creating intimidating environments that hinder effective treatment. Transitions, whether related to admission, transfer, or discharge, were frequently associated with fear, particularly in cases involving police presence. Poor communication and a lack of involvement during these transitions exacerbated negative experiences for patients, highlighting the urgent need for improvements in these critical processes.
Exploring Individual Experiences: Autonomy and the Impact of Trauma
The concept of ‘the individual’ encompasses the infringements on autonomy that patients face, along with the potential (re)traumatization stemming from their cumulative adverse experiences. Life on a mental health ward often results in patients feeling a profound loss of control, privacy, freedom, power, and choice, all of which contribute to their negative experiences. Patients frequently report a lack of agency regarding admission and treatment choices, physical barriers such as locked doors, and restrictions on daily activities like mealtimes and bedtimes. They also experience limitations regarding personal items and perceive a significant power imbalance between themselves and the staff. Consequently, many patients express feelings of coercion and infantilization, where they are provided with false choices rather than genuine autonomy. Throughout the literature, it is evident that patients frequently describe their experiences on inpatient wards as traumatic, with additional factors such as gender, abuse, and racism further complicating their situations.
The review found a range of factors related to adverse inpatient experiences, suggesting that traumatic experiences in inpatient settings can worsen outcomes.
Insights from the Review: Comprehensive Understanding of Adverse Experiences
This systematic review has illuminated that adverse experiences in inpatient mental health settings are multifaceted and extend beyond the harm inflicted by restrictive interventions. It highlights the intricate interplay between systemic, environmental, and individual factors that contribute to these detrimental experiences. Notably, while the challenges posed by these factors are significant, the review also underscores the substantial opportunities available for enhancing mental health inpatient care.
Strengths and Limitations of the Review: A Balanced Perspective
The review draws upon a diverse array of studies from multiple countries, focusing specifically on adverse inpatient experiences and addressing a critical gap in the literature. It provides a valuable framework for mapping and addressing these negative experiences, offering practical insights for various stakeholders. Importantly, the research benefited from the meaningful involvement of individuals with lived experience throughout the project, ensuring that the findings resonate with real-world perspectives.
Nevertheless, certain limitations must be acknowledged. A significant portion of the studies included were conducted in Europe, and only studies published in English were considered, which may restrict the applicability of the findings to other mental health systems. Additionally, specialized settings, such as inpatient services for children and young people, individuals with learning disabilities, and older adults, were excluded, potentially limiting the relevance of the findings for these groups.
While the application of ecological systems theory provided a valuable framework for interpreting the findings, it does have limitations. The review did not extensively examine variations in outcomes across different settings and populations, such as differences between countries, ward types, or patient demographics. Therefore, while the framework is broadly applicable to inpatient mental health services, it may not fully capture the unique nuances present in specific contexts and populations. Furthermore, the boundaries between system levels can sometimes be ambiguous, and the relative influence of different layers may fluctuate across cultural contexts and over time—elements that could warrant further exploration in the paper.
The review authors also noted that few of the included studies explicitly focused on adverse experiences beyond those associated with restrictive interventions. This may leave certain dimensions of patients’ experiences underrepresented. The complexity of conducting a comprehensive investigation is also heightened by the lack of a consistent definition of “adverse experiences” within the literature, along with the varied methodologies employed in studying and measuring these experiences.
Research findings are influenced not only by how adverse experiences are defined but also by the study designs utilized, including data collection and analysis methods. Many studies included in the review showed a lack of transparency regarding the nature of interviewer-participant relationships, which made it challenging for reviewers to assess potential biases. Although the reviewers examined patient quotes in the original studies to mitigate selective reporting, such biases may still exist, potentially impacting the representation of patients’ experiences, especially given that most studies did not include patient co-researchers.
Finally, the review’s focus on adverse experiences serves as both a strength and a limitation, as it addresses an important but often overlooked area. However, this focus may inadvertently overlook the rich complexity and diversity of patients’ experiences within inpatient settings. Many individuals may have both negative and positive experiences; what is harmful for one person might be beneficial for another. A more balanced approach that considers both positive and negative experiences could yield a more comprehensive understanding of inpatient care. Capturing the full spectrum of patient experiences would accentuate not just the factors that cause harm, but also those that facilitate recovery, thereby further guiding improvements in inpatient mental health services.
Adverse experiences were not consistently defined across included studies and few of them explicitly examined adverse experiences.
Practical Implications: Transforming Inpatient Mental Health Care
The framework developed from the findings of this review serves as a valuable tool for a diverse range of stakeholders, including academics, clinicians, commissioners, and policymakers, aiming to better understand and address adverse experiences within inpatient mental health settings. It underscores the interconnectedness of individual, relational, and societal factors influencing inpatient care. By addressing the comprehensive spectrum of adverse experiences identified, mental health services can make significant strides toward creating environments that not only prevent harm but actively foster the wellbeing and recovery of the individuals under their care.
The review’s emphasis on systemic factors in shaping patients’ experiences is crucial, as it challenges the prevalent notion that recovery is predominantly a matter of individual resilience. This critical perspective is encapsulated in the authors’ poignant question:
How can someone expect to recover, or at least improve to the point of discharge, when they are surrounded by an ecosystem, and the associated processes and transitions, that create adversity?
Recognizing the significance of these broader contexts shifts the focus from expecting individuals to merely cope better to advocating for essential structural changes within inpatient services aimed at minimizing harm.
Achieving meaningful change in inpatient mental health care is likely to be a complex endeavor that necessitates consideration of various factors and perspectives. It is plausible that some adverse experiences may be inevitable within the current system, particularly when patients’ rights are constrained, and universally applicable solutions might not exist. However, the findings of this review present a valuable starting point for fostering dialogue among patients, caregivers, healthcare professionals, and policymakers to deepen their understanding of how inpatient care impacts patients. These insights can inform actions aimed at reducing harm and enhancing care at all levels:
At the individual level (e.g., by enhancing patient choice, control, and freedom),
Within systems (e.g., by minimizing coercive practices and improving admission/discharge protocols),
In ecosystems (e.g., by upgrading physical ward environments and boosting patient involvement), and
In broader policymaking (e.g., by influencing national policies and best practice guidelines).
Together, these efforts could create a more inclusive, patient-centered inpatient care model that is less traumatizing, ultimately reducing harm and enhancing care throughout the entire system.
The findings of this review further underscore the importance of involving individuals with lived experience at every stage of future research—from formulating research questions and designing studies to collecting and analyzing data and disseminating findings. Engaging these individuals would ensure that future research better aligns with their priorities, perspectives, and lived experiences. Additionally, collaborating with those who have navigated inpatient mental health care could facilitate the development of a more inclusive and standardized definition of “adverse experiences.” This would enable future research to adopt a more consistent and comprehensive approach to studying these experiences and examining changes over time.
Future investigations could also explore how the proposed framework can be adapted to different contexts, such as varied ward types, geographic locations, and patient demographics. Realist approaches could be employed to further dissect the mechanisms linking these factors to outcomes, investigating what works (or doesn’t), for whom, in what circumstances, and why. This information would be invaluable for stakeholders aiming to implement more effective, evidence-based strategies to prevent harm and promote positive outcomes across diverse inpatient settings and populations.
By addressing the full spectrum of adverse experiences, mental health services can make strides towards environments that not only prevent harm, but actively contribute to the wellbeing and recovery of individuals in their care.
Hallett, N., Dickinson, R., Eneje, E., & Dickens, G. L. (2024). Adverse mental health inpatient experiences: Qualitative systematic review of international literature. International Journal of Nursing Studies, 161, 104923. Advance online publication. https://doi.org/10.1016/j.ijnurstu.2024.104923
Astrid Moell, Maria Smitmanis Lyle, Alexander Rozental, Niklas Långström, 2024 Rates and risk factors of coercive measure use in inpatient child and adolescent mental health services: a systematic review and narrative synthesis, The Lancet Psychiatry, https://doi.org/10.1016/S2215-0366(24)00204-9.
Griffiths, J. L., Saunders, K. R. K., Foye, U., Greenburgh, A., Regan, C., Cooper, R. E., Powell, R., Thomas, E., Brennan, G., Rojas-García, A., Lloyd-Evans, B., Johnson, S., & Simpson, A. (2024). The use and impact of surveillance-based technology initiatives in inpatient and acute mental health settings: a systematic review. BMC Medicine, 22(1), 564. https://doi.org/10.1186/s12916-024-03673-9
Bronfenbrenner, U. (2005). Ecological systems theory (1992). In U. Bronfenbrenner (Ed.), Making human beings human: Bioecological perspectives
Ann Miller is a certified mental health coach and wellness writer with a strong background in psychology and emotional resilience. With over a decade of experience in helping individuals manage stress, anxiety, and burnout, Ann specializes in making complex mental health topics accessible and empowering.
She holds a Master's degree in Clinical Psychology and has worked with both individual clients and organizations to promote emotional well-being and work-life balance. Through her writing, Ann aims to break the stigma surrounding mental health and offer practical, compassionate guidance for everyday challenges.
When she's not writing or consulting, Ann enjoys early morning yoga, quiet reading time, and exploring nature trails with her dog. Her personal philosophy: "Mental health is not a luxury — it’s a foundation for everything we do."
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept All”, you consent to the use of ALL the cookies. However, you may visit "Cookie Settings" to provide a controlled consent.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checkbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checkbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.













 Surveillance in Inpatient Mental Health Settings: Impact and Use
Surveillance in Inpatient Mental Health Settings: Impact and Use